The Healthy Opportunities Pilot
While access to high-quality medical care is critical, research estimates that up to 80% of health outcomes that can be altered are related to social determinants of health,1–3 or “the conditions in the environments where people are born, live, learn, work, play, worship, and age.4” The United States spends approximately 95% of its health budget on direct medical care, with only 5% going to population health efforts,5 suggesting that the country is currently buying health care, but not necessarily buying health. In 2017, the North Carolina Department of Health and Human Services (NCDHHS) began its comprehensive strategy to buy health through its Healthy Opportunities efforts.
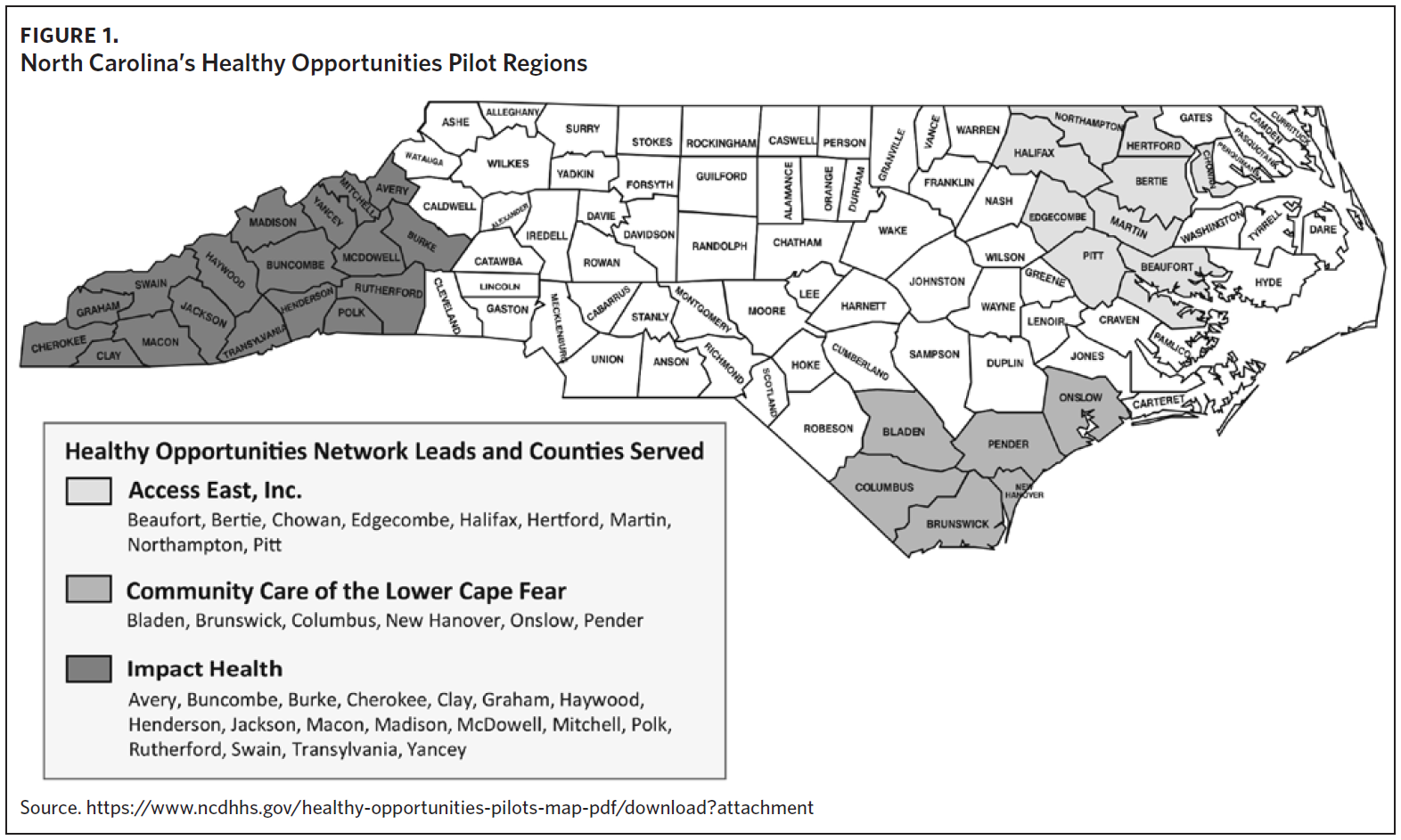
In October 2018, as a part of its 1115 Medicaid Demonstration waiver,6 NCDHHS received federal authority to spend up to $650 million in state and federal Medicaid funds to address the health-related resource needs of NC Medicaid enrollees in three regions of the state through the Healthy Opportunities Pilots (HOP).7 Up to $100 million can support infrastructure development for human service organizations (HSOs, also known as community-based organizations or social service agencies) to allow them to serve more individuals. Most funds are used to reimburse for a select set of 29 evidence-based, federally approved non-medical services for eligible Medicaid enrollees.8 To assist most HSOs with operating as Medicaid providers for the first time, NCDHHS procured “Network Lead” organizations, which connect HSOs to health plans and offer HSOs technical assistance and training. NCDHHS is employing a comprehensive evaluation design to test whether HOP services improve health outcomes and reduce overall health care costs for Medicaid enrollees.9
Perhaps the most notable aspect of HOP is the scale of the services and populations covered. Prior to HOP, some state Medicaid programs reimbursed for a narrow set of non-medical services (e.g., home-delivered meals) for small sub-populations (e.g., enrollees in the Community Alternatives Program for Disabled Adults). However, HOP is the country’s first comprehensive program to reimburse for such a broad set of services (addressing food/nutrition, housing/ utilities, transportation, and interpersonal violence/toxic stress needs) for a broad array of Medicaid populations with Medicaid funds (including children, pregnant individuals, and adults with both medical and non-medical needs).10 It is also the country’s first Medicaid program to reimburse for non-medical services using a fee schedule.
Early Findings from Nearly Two Years of the Healthy Opportunities Pilots
Recognizing that HOP was a new and innovative program, NCDHHS strategically launched its services in phases, starting with food/nutrition in March 2022 before expanding to housing/utilities and transportation in May 2022, toxic stress in June 2022, and interpersonal violence services in April 2023. This approach allowed NCDHHS and its partners to quickly identify and address challenges and act on opportunities.11
As of January 2024, HOP has delivered over 265,000 services to over 20,000 enrollees and their families in predominantly rural areas of North Carolina.12 These services translate into over $47 million in reimbursement to North Carolina’s local HSOs. The program is also operating efficiently, with 95% of service authorizations approved and 93% of invoices accepted, paid, or in progress.13
Unlike most traditional Medicaid services, HOP services can support the enrollee as well as their family. For example, a mother of two who has a high-risk pregnancy and is food insecure may be eligible for a large healthy food box meant to support both her and her children. This recognizes that if one individual in a family is food insecure, the whole family is likely food insecure, and that parents often ensure their children are fed before feeding themselves. Similarly, if a child with asthma is housing insecure and eligible for HOP, the child may be eligible for carpet cleaning or mold removal services, which benefit the entire family. HOP enrollment numbers only reflect HOP enrollees, but their families benefit from these services as well.
Somewhat surprisingly, the loss of Medicaid due to continuous coverage provisions ending at the end of the public health emergency seems to have had limited impact on access to HOP services.14 Medicaid expansion, implemented in December 2023, already shows promise for increasing access to HOP services, with over 100 Medicaid expansion members enrolled in HOP in the first week.15

Another unique aspect of HOP is its service definitions. While some services are narrowly defined (e.g., one month’s rent and security deposit), others are flexible, allowing services to meet individuals’ and families’ needs. For example, Healthy Home Goods can cover an array of services to reduce home-based health and safety risks, including air filters, hypoallergenic mattresses or pillow covers, or pest control supplies. Healthy Food Boxes can be tailored to be culturally sensitive and age appropriate (e.g., including infant formula) and many boxes come with recipes and nutrition education materials. Some HSOs have even set up food delivery vans that go to the enrollee’s home and allow the enrollee to select the contents of their Healthy Food Box. Reimbursement for private transportation, which can be used for ridesharing apps or community transportation options, can also be used for repairs to an enrollee’s vehicle or reimbursement for gas mileage. These customizable services have allowed families to receive services that uniquely meet their needs.
In March 2023, NCDHHS released the results of its first rapid cycle assessment (RCA) as part of its Centers for Medicare and Medicaid Services (CMS) evaluation.16 RCAs are intended to provide early learnings that can be used to adapt the pilot design and fee schedule before the final, summative evaluation. Results from the first RCA only include 1.5 years of infrastructure-building data and eight months of service-delivery data, so results are extremely preliminary. Some of the key findings demonstrated17:
-
Network Leads and HSOs report benefits from HOP participation, including building networks of collaboration, supporting growth of HSOs, and improving community health and wellness;
-
63% of HOP enrollees received at least one invoiced service, with more in the pipeline for delivery;
-
Food services constituted the majority (90%) of services delivered;
-
Over 75% of services had a service start date within two weeks of HOP enrollment, showing that enrollees are getting services quickly;
-
Invoices for services were paid timely: 56% of invoices were paid within 30 days, 90% within 60 days, and 98% within 90 days;
-
Needs are highest around the time of HOP enrollment (mean of 1.73 needs) with slight decrease over time (mean needs after 90 days: 1.68);
-
Intervention effects may vary across service domain types, e.g., risk of reporting a food need at 90 days was slightly lower with delivered meals compared to food subsidies (e.g., fruit and vegetable prescriptions).
Perhaps more meaningful than the numbers are direct accounts from Medicaid enrollees of the impact that HOP has had on their lives. One enrollee, Dawn Verret, lost her job at the beginning of the pandemic and then was hospitalized in November 2020 for malnutrition and neuropathy, and again in June 2022 for pneumonia. Her health plan sent a caseworker to visit her mobile home outside of Asheville, saw the conditions that Dawn was living in, and recommended her for HOP. Dawn, who had not been able to take a full shower since she was in the hospital, was able to have her deteriorating bathroom renovated and covered by HOP. After the project was complete, Dawn stated, “I really believe that I’m gonna be able to take care of myself and get stronger because I feel like I’m my best self… You have no idea what being able to take a shower every day does to your self esteem.18”
Successes, Challenges, and Lessons Learned to Date
Inherent in HOP’s design is its commitment to learning and continuous quality improvement. Some of the most significant accomplishments in the past two years have been the learnings gained and shared. These learnings will not only improve HOP for its participants but can help other states that are currently implementing similar initiatives.19,20
Early and Frequent Partner Engagement
Vital to HOP’s success is NCDHHS’s early and frequent engagement with its partners. From initial design of the HOP fee schedule to current troubleshooting of operational issues, NCDHHS has proactively sought input from its health plan, care management entity, Network Lead, and HSO partners. Together, we have been able to enhance a number of HOP features in the past two years, including:
-
Increasing the number of members served through HOP, through methods including a time-limited, data-driven, presumed eligibility pathway and text message campaign; funding for HSOs to conduct grassroots community engagement; the creation of a “No Wrong Door” referral in NCCARE360, where any user can refer a Medicaid member to HOP; and a communications toolkit and campaign;
-
Streamlining the HOP enrollment and consent process;
-
Continually enhancing NCCARE360 for HOP, including automated HOP enrollment and service authorization functionalities and continuous improvements to invoicing functionality;
-
Housing service simplifications, including eliminating unnecessary documentation for enrollees and providing additional housing coordination payments to HSOs;
-
Adding HOP eligibility criteria, most recently to expand HOP eligibility to Medicaid Direct enrollees and including new eligibility criteria such as chronic infectious disease, cancer, and autoimmune disorders;
-
Finding a safe and secure way to offer services to HOP enrollees experiencing interpersonal violence.
Importance of Network Leads and Standardized Contracts
Network Leads are fundamental to the success of the HOP. They have helped HSOs learn how to navigate the Medicaid system, redesign certain business processes, and expand their scope of services. This has been particularly important in ensuring that smaller, less resourced HSOs can participate in HOP. Network Leads also serve as a resource to health plans by providing them with a high-quality network of HSOs. State-developed standard contracts between health plans and Network Leads21 and Network Leads and HSOs22 ensure clear responsibilities across parties and help balance power dynamics that could potentially over-medicalize HSOs.
Training and Technical Assistance
Embedding non-medical services and providers into Medicaid helps address whole-person health, but also requires new ways of working for all entities. Robust training and technical assistance tools for both the medical and non-medical sectors have proved extremely beneficial. Network Leads have developed multiple tools to help HSOs enroll as Medicaid providers, bill for services, and meet program integrity requirements. NCDHHS and its partners have developed in-depth trainings for care management entities and prepaid health plans (PHPs) that detail the non-medical services provided through HOP and best practices for addressing social needs.23
Shared Data and Technology
The use of one shared technology platform by all HOP-participating entities has been necessary for sharing data needed to operate and evaluate HOP. Creating a simple invoicing solution for HSOs has made it possible for many of them to participate in HOP; translating invoices to encounters streamlines the evaluation of medical and non-medical data, and having only one system reduces the need for organizations to use multiple technologies, creating broader partnerships.
Looking Ahead
As HOP continues, NCDHHS intends to expand HOP services to new populations. With recent approval from CMS to cover HOP for Medicaid Direct populations,24 NCDHHS will phase in access to HOP services for this population, beginning with those eligible for Tailored Care Management, in 2024. Tailored Plan enrollees can access HOP services when Tailored Plans are live in 2024.
Additionally, NCDHHS is seeking authority from CMS to expand coverage of HOP services statewide. North Carolina’s current 1115 waiver demonstration ends in October 2024. NCDHHS has submitted a request to CMS to renew and amend its current waiver in the next demonstration period (November 2024 to October 2029).25 Through this request, NCDHHS is seeking to expand coverage of HOP services statewide, procure new Network Leads to cover new regions of the state, scale and modify certain existing HOP services, and further expand HOP eligibility criteria.
NCDHHS will continue to closely monitor and evaluate the HOP program during the current and future waiver periods and is committed to continually enhancing the program based on learnings and feedback. North Carolina has been setting a precedent for the country on addressing healthy opportunities in Medicaid and looks forward to continuing to lead the way.
Acknowledgments
No conflicts of interest were disclosed.